Intern/RMO1 membership
Start practising with confidence, knowing your career and health are protected

Support, when you need it most
Embarking on your first years as a doctor will provide many opportunities to develop your skills.
Practise with confidence with FREE Avant medical indemnity insurance for interns/RMO1s, which includes cover for civil liability, legal fees and disciplinary or coronial inquiries.
As a member you'll have access to Avant’s expert medico-legal advisers to help you whenever you need it, 24/7 in an emergency. As well as access to award-winning Avant Law, Australia’s largest in-house medico-legal team. Which is important if there are situations where your hospital cover doesn't protect you.

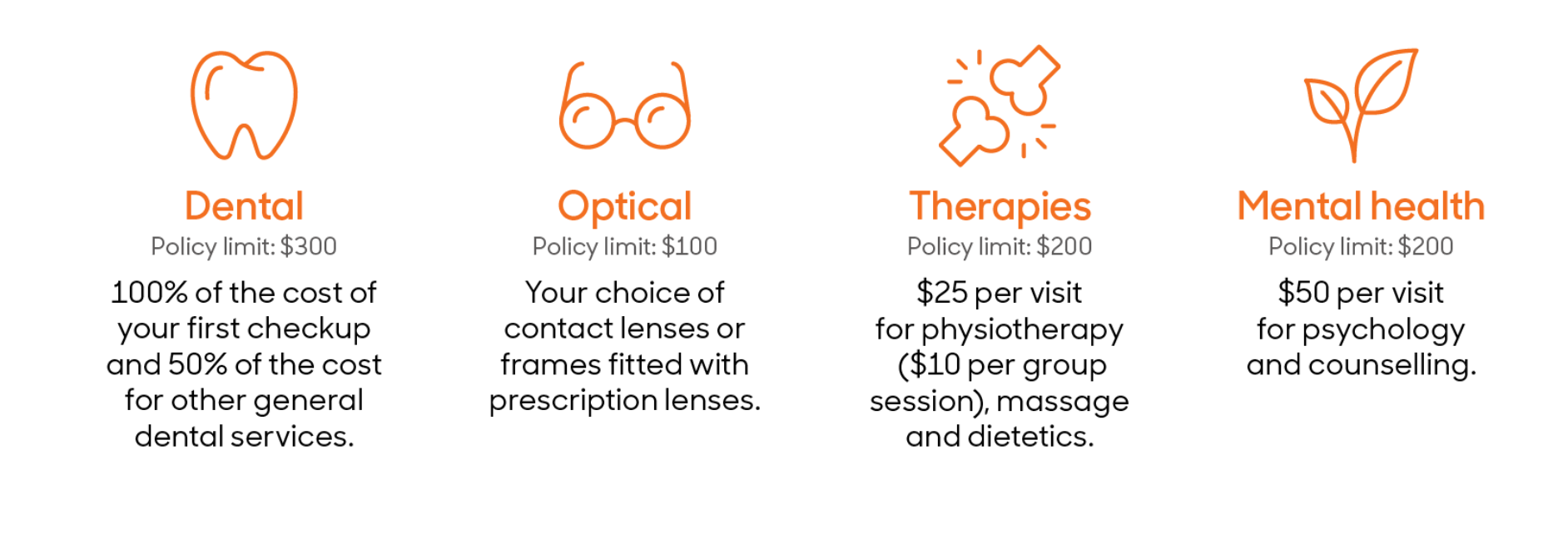
Lite Extras Cover has been designed to introduce you to the benefits of private health insurance without the financial burden of having to pay a premium. Claim benefits for services like dental, optical, physio and more from 1 January to 31 December 2024. For more details visit doctorshealthfund.com.au/liteextrascover.
If you're an Avant member, make sure we have your up-to-date personal details to ensure you receive your Lite Extras Cover.
Lite Extras Cover benefits:
In addition to FREE medical indemnity insurance and FREE Lite Extras Cover, intern/RMO1 members also receive these great benefits:
Avant Advocacy
Avant uses its position to advocate on issues affecting doctors, providing a respected voice in an increasingly complex environment.
Avant Member Grant Program
Access to funding for research with a special focus on supporting early career researchers.
Medico-legal Advisory Service
Specialist medico-legal advisers available 24/7, in emergencies, to offer advice and support.
Insights and resources
Educational resources for your specialty
Avant Law Medical Indemnity
With Australia’s largest medical indemnity team.
Early Career Doctor Advisory Council
A group of your peers advising Avant of emerging and existing issue facing junior doctors today.

Cover is subject to approval and to the terms, conditions and exclusions of the policy. To decide if a policy is right for you, please carefully read the relevant Product Disclosure Statement (PDS), which is available here or by contacting us on 1800 128 268.
^Lite Extras is a private health insurance product issued by The Doctors’ Health Fund Pty Limited, ABN 68 001 417 527 (Doctors’ Health Fund), a member of the Avant Mutual Group. Unless you advise us that you do not wish to accept the offer, as part of your Avant membership you will receive a fully subsidised Lite Extras policy from Doctors’ Health Fund. If you do not wish to receive this offer please opt out here. Doctors’ Health Fund will collect and use the personal information provided on your Avant membership to issue and administer your Lite Extras policy. For more information and terms & conditions visit www.doctorshealthfund.com.au/liteextrascover or to view our privacy policy visit www.doctorshealthfund.com.au/privacy-policy.
*IMPORTANT: The information provided in this material is general advice only and has been prepared without taking into account your objectives, financial situation and needs. You should consider these, having regard to the appropriateness of this advice as well as the Product Disclosure Statement and Target Market Determination before making a decision to acquire a financial product. You should also read our Financial Services Guide for detail about who we are, how we are remunerated and how our Doctors Life Insurance Selection Tool (LIST) works. For further important information please see Avant - Life insurance for doctors . The LIST is provided by Avant Life Insurance. “Avant Life Insurance" is a registered business name of Doctors Financial Services Pty Ltd ABN 56 610 510 328 AFS Licence Number 487758 (DFS).

See offer page for more information.


